
MPLT: Antipsychotic Efficacy Is the Floor. Tolerability Is the Trade Into Ph2 Readout
Cobenfy proved dual M1/M4 agonism works. Ph2 ZEPHYR's job is showing whether ML-007C-MA's PK-tuned tolerability edge is real — which is why the AE table, not the PANSS table, carries the real signal.

I. The Muscarinic Class's Second Mover
Branded antipsychotics (aka SGAs) are entering a new phase. Two decades of dopamine-based atypicals have given way to a wave of differentiated launches — Lybalvi, Caplyta, and most consequentially, Cobenfy — that compete on tolerability and treatment persistence, not incremental receptor pharmacology. Cobenfy’s September 2024 approval validated M1/M4 agonism after decades of failed attempts, materially lowering the biological risk for the class. The investment debate has moved on from there.
MapLight’s Ph2 ZEPHYR trial asks a narrower, more commercially relevant question. ML-007C-MA doesn’t need to prove muscarinic agonism works — it needs to show that a PK-tuned pairing of ML-007 with fesoterodine preserves Cobenfy-like efficacy while meaningfully reducing the GI adverse events, titration complexity, and dosing friction constraining broader adoption.
Neuropsychiatric readouts carry more uncertainty than most therapeutic areas, and investors typically treat them as binary efficacy events. That framing is largely outdated here: Cobenfy-like efficacy is a reasonable base case, not the central uncertainty — though we lean conservative within that range, expecting replication at the low end of the EMERGENT band, not mid-band. The real value driver isn’t the PANSS table, it’s whether the AE profile validates MapLight’s PK synchronization hypothesis at scale — and our own review of the Ph1 and comparator data leaves us short of conviction on that claim this early, directionally supportive but not yet definitive. Get both right, and the debate shifts from mechanism validation to commercial differentiation, with implications reaching well beyond schizophrenia into the larger Alzheimer’s disease psychosis opportunity.
II. Cobenfy Changed the Bar, Not the Opportunity
Cobenfy settled the muscarinic biology question in acute psychosis. It did not settle whether reducing cholinergic side effects actually changes prescribing behavior — the assumption MapLight’s pitch rests on.
Before Cobenfy’s Sep 2024 approval, the open question wasn’t whether muscarinic agonism worked — xanomeline’s antipsychotic activity had been suggested in small studies going back to the late 1990s and 2000s, though never in a large, well-powered trial. KarXT’s own Ph2 (EMERGENT-1) had already cleared its primary endpoint with a strong effect size (Cohen’s d 0.75) back in 2020. But replication risk remained: whether that signal would hold at Ph3 scale, given how often psychiatric trials see Ph2-to-Ph3 attenuation. It did — EMERGENT-2 and EMERGENT-3 replicated with similar effect sizes (d 0.61, 0.60) and placebo-adjusted PANSS improvements of ~9-10 points across all three trials (~750 patients), enough for approval as the first genuinely new schizophrenia mechanism in three decades. That question is closed. Investors evaluating ML-007C-MA are no longer underwriting receptor biology or replication risk; they’re underwriting formulation, execution, and whether a tolerability edge translates into commercial share.
None of this happens in a vacuum of unmet need. An estimated 30% of schizophrenia patients meet criteria for treatment resistance — inadequate response to at least two antipsychotic trials — and real-world surveys of US psychiatrists put a comparable share of their caseloads in that category. For this population and the broader group with residual symptoms on existing therapy, a genuinely novel mechanism carries weight independent of its side-effect profile.
Cobenfy also showed where the muscarinic agonist class still struggles. It avoids the metabolic, prolactin, and movement-disorder liabilities that have constrained D2-blocking antipsychotics for decades — genuinely differentiated, durable advantages. What it didn’t avoid is an early, largely transient cholinergic AE burden: TEAE rates ran well above placebo across the pivotal program (52% vs. 40% in EMERGENT-1, with similar gaps in EMERGENT-2/3), driven mostly by GI events — nausea, constipation, vomiting, dry mouth — concentrated in the first week and rarely leading to discontinuation (D/C). Add BID dosing with a week of titration, and the friction is real, even if survivable for most patients.
Whether that friction actually limits adoption is the assumption worth questioning, not accepting. MapLight’s pitch implicitly treats “fewer peripheral AEs” as equivalent to “better commercial uptake.” Schizophrenia prescribers routinely tolerate drugs carrying chronic weight gain, diabetes risk, and irreversible movement disorders in exchange for efficacy and manageability — against that bar, a few days of nausea or constipation may be a favorable trade, particularly for patients who’ve already cycled through multiple generic antipsychotics. Cobenfy’s actual launch trajectory supports this read: worldwide net sales have grown steadily since the partial Q4’24 launch quarter — a linear expansion (FY25 $155M) rather than a hockey-stick inflection — tracking close to consensus at most checkpoints rather than badly missing on tolerability-driven hesitancy. BMS has attributed the pace to formulary access, field-force build-out, and the slow work of breaking entrenched D2-antagonist prescribing habits — less to patients or physicians balking at GI side effects. Better GI tolerability and better prescribing behavior are not the same claim, and this note treats them as separate hypotheses throughout.
For MapLight, matching Cobenfy’s efficacy is the entry price, not the differentiator (see Section IV). The real test is whether PK synchronization reduces treatment-limiting cholinergic toxicity specifically, not just AE incidence broadly, while holding efficacy — a materially higher bar than beating Pbo.
MapLight isn’t racing the Cobenfy that launched in 2024 — it’s racing the more established, better-adopted Cobenfy likely to exist by the time ML-007C-MA could reach the market.
The field has already run the alternative experiment, and it didn’t work — but not on safety. Selective M4-only agonists (emraclidine) bet that isolating M4 activation could preserve efficacy while eliminating M1-driven peripheral effects; the program missed on efficacy against an unexpectedly strong placebo response, not on tolerability — a distinction the market tends to skip past. Paired with preclinical knockout data showing that removing either M1 or M4 shifts potency without eliminating efficacy, both receptors appear mechanistically necessary — meaning the next real differentiation in this class won’t come from re-litigating receptor selectivity. It comes from medicinal chemistry and PK engineering, which is exactly the bet MapLight is making.
III. The Tolerability Bet: Can Better PK Actually Fix Cobenfy’s AE Problem?
MapLight isn’t claiming to eliminate the cholinergic side effects that limited Cobenfy — it’s claiming to shift which ones show up, by tuning the ratio between agonist and peripheral blocker rather than just co-administering the two. Multiple Ph1 studies partially support that claim — but only the narrower version of it, not the stronger one.
IIIA — What “PK synchronization“ actually means
Cobenfy established that pairing a muscarinic agonist (xanomeline) with a peripheral anticholinergic (trospium) makes an old, previously untenable mechanism commercially viable. The original proof-of-concept for this pairing showed something specific: trospium didn’t lower xanomeline’s systemic exposure — plasma levels were essentially unchanged — yet cholinergic side effects fell sharply. The benefit came from trospium physically blocking peripheral muscarinic receptors, not from reducing how much drug reached the body. That’s the class’s founding mechanism.
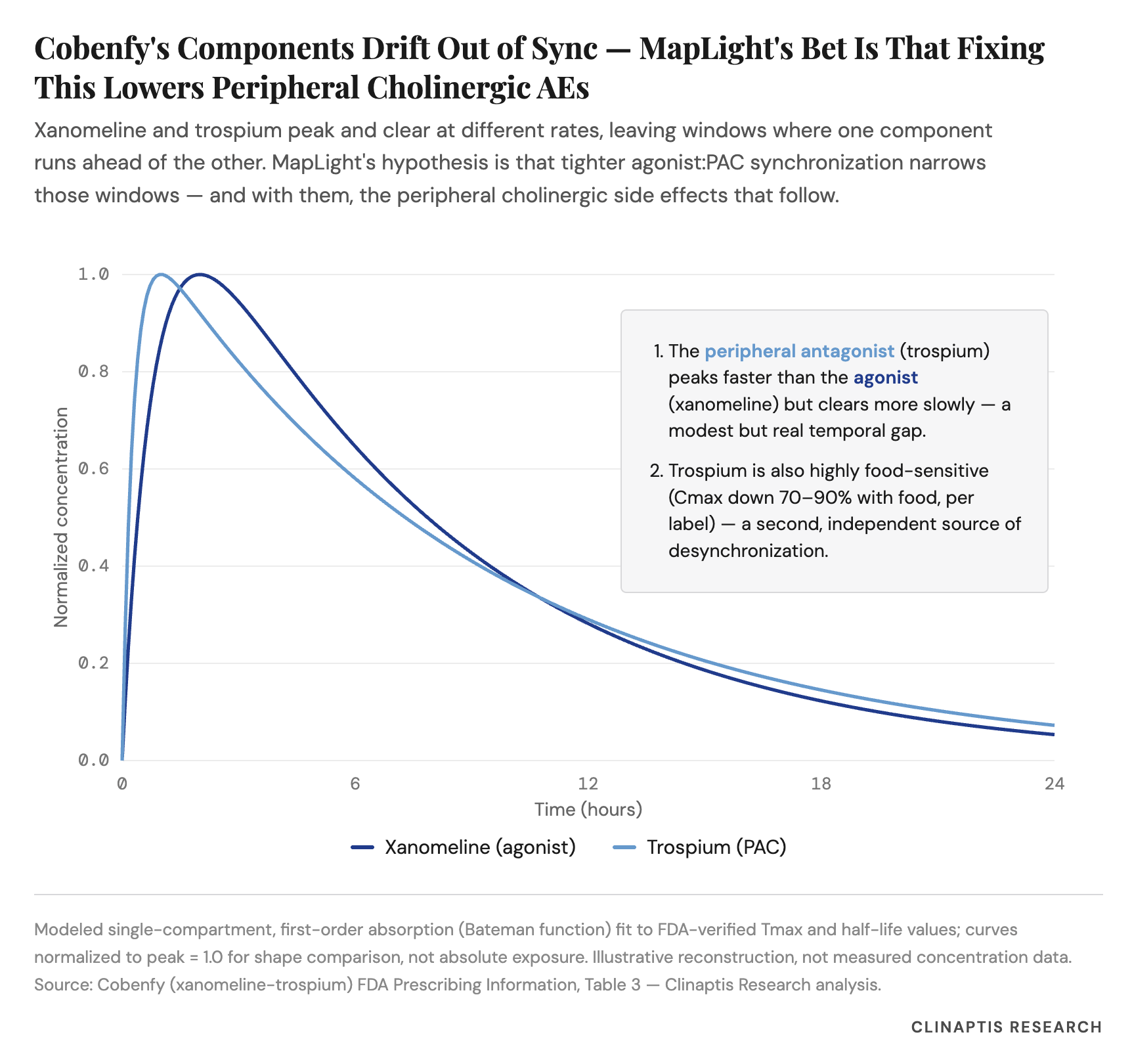
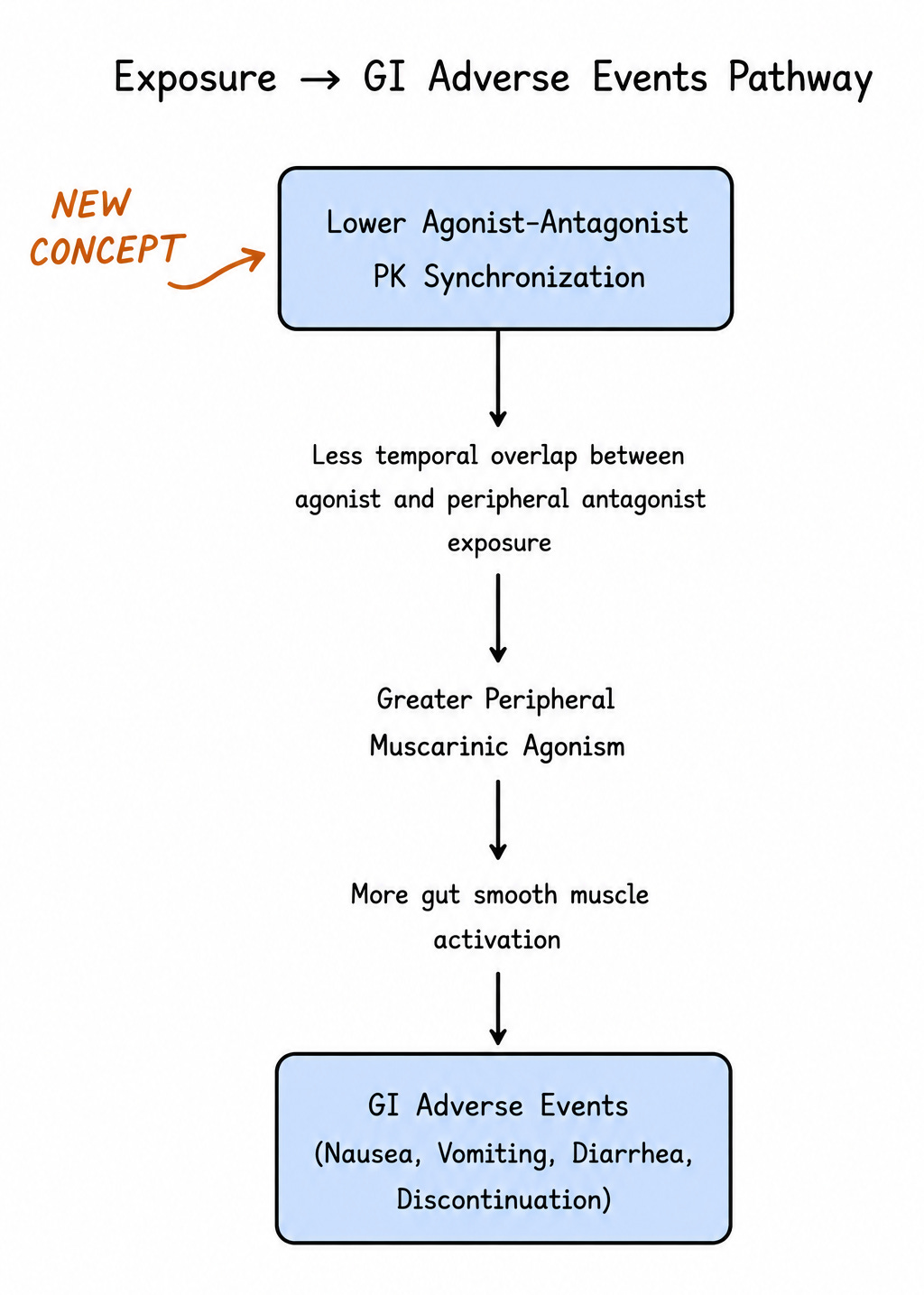
MapLight’s pitch is a layer on top of that, not a repeat of it: peripheral tolerability isn’t just about whether you block peripheral receptors, but how precisely the blocker’s exposure tracks the agonist’s, over time. Picture two runners on a track. If the agonist gets ahead, peripheral receptors fire unopposed — nausea, vomiting, sweating. If the blocker gets ahead, the opposite problem appears — dry mouth, constipation, blurred vision. MapLight’s engineering choice — fesoterodine in place of trospium, precision-matched to ML-007’s exposure curve — aims to keep the two “runners” together longer, via a target plasma ratio window of 100:1 to 600:1 (ML-007:PAC). Fall below that window and anticholinergic effects dominate; rise above it and procholinergic effects take over.
This is a Goldilocks-zone hypothesis, not an elimination hypothesis. Nobody is claiming to turn off the underlying cholinergic biology — the claim is narrower: keep it inside a tighter band than Cobenfy managed.
IIIB — What the evidence actually shows
The company’s own Ph1 data, at the two doses now carried into Ph2 ZEPHYR (210/3 mg BID and 330/6 mg QD), gives a mixed but interpretable picture next to Cobenfy’s FDA-reviewed safety data:
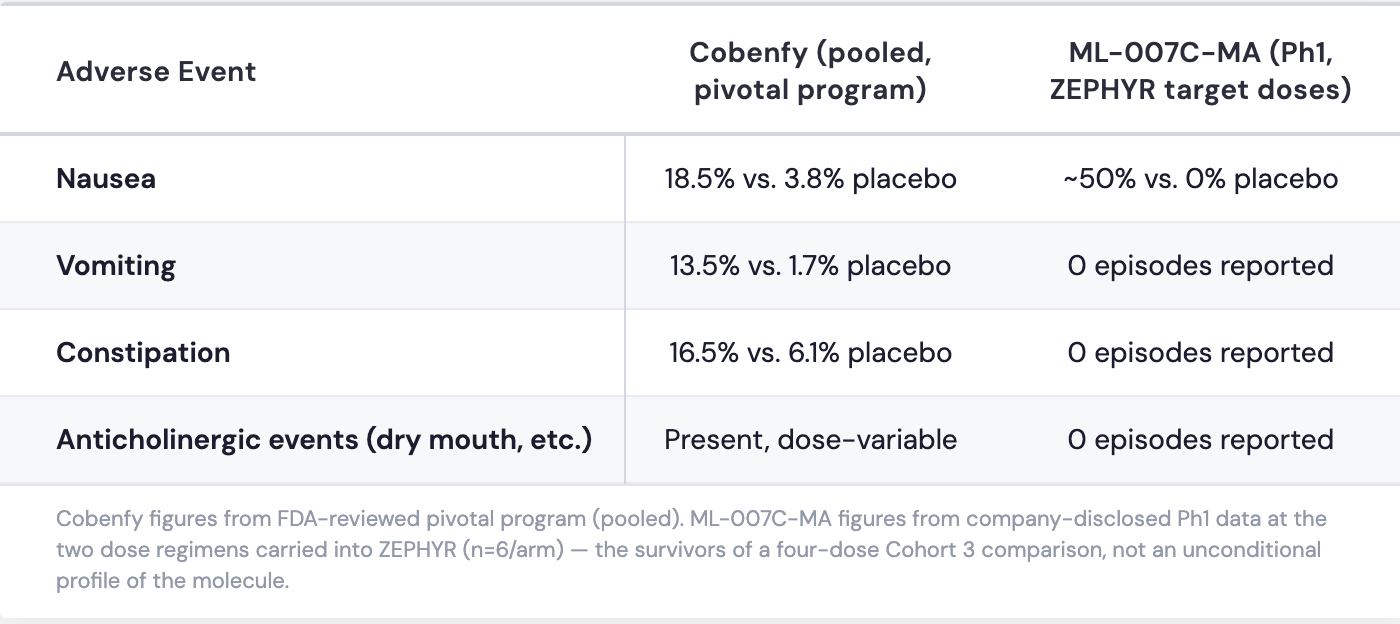
Read plainly: this is not “fewer AEs across the board.” Nausea shows up in half the ML-007C-MA cohort at target dose — unremarkable-to-elevated on its own. What’s different is the composition: no vomiting, no constipation, no anticholinergic events, against a Cobenfy program where all four categories were elevated versus Pbo. If this pattern holds at scale, the commercial argument is coherent: persistent nausea for a few days is a tolerable nuisance, while vomiting and constipation are more likely to drive discontinuation — and discontinuation, not mild GI discomfort, is what actually limits real-world antipsychotic (AP) use. That’s a distinguishable claim from “we solved cholinergic toxicity,” and a more credible one.
IIIC — The caveats, stated plainly
First, the clean doses are survivors, not an unconditional profile. The Ph1 study that produced this data tested four dose regimens; two (165/3 BID and 270/6 QD) aren’t shown in the disclosed tables (to our knowledge), and regulatory disclosures confirms vomiting and constipation did occur somewhere across the four regimens tested. The two ZEPHYR doses are, by construction, the cleanest of four tested — good evidence of successful dose selection, weaker evidence the molecule is inherently free of these events.
Second, small samples move a lot with single events. Six patients / arm means one patient shifts an incidence rate by ~17 points. Nausea at 50% and dizziness at 50%/33% across the two doses show no clean dose-ordering at the individual-AE level — the same noisy, non-monotonic pattern that showed up in Cobenfy’s own FDA exposure-response analysis, where higher exposure didn’t track with higher AE rates either. Neither dataset yet supports a precise, mechanistic dose-response story.
Third, cross-program comparisons of this kind are inherently approximate — different molecules, populations, trial eras, and formulations. The table above is directionally informative, not statistically rigorous, and that caveat applies to every AE comparison in this note.
Deeper dive into hepatic chemistry (skip if not interested in the mechanism weeds) FDA’s review of KarXT flagged a modest excess of liver enzyme elevations, with one hypothesis being that some reflected transient cholinergic-induced biliary spasm rather than classic drug-induced liver injury. Structural comparison of ML-007 against xanomeline shows the two molecules differ substantially in lipophilicity and protein binding, and one computational model predicts markedly lower inhibition of BSEP — the bile transporter specifically implicated in cholestatic liver injury (source: ADMETlab 3.0). Predicted overall liver-injury risk scores were similar for both molecules, so this is a specific point of chemical differentiation worth flagging, not evidence of lower clinical hepatotoxicity. Actual clinical liver-safety data from Ph2/3 will be the real test.
IV. Reading Ph2 ZEPHYR’s Efficacy Data: A Calibration Band, Not a Pass/Fail Line
ZEPHYR and EMERGENT-1 are close to the same trial run twice — same population, design, endpoint, and a majority of the same sites (ct.gov analysis) — which makes cross-trial calibration relatively more defensible here than the standard caveat usually allows.
ZEPHYR is best read as an evolution of EMERGENT-1, not an independent trial that happens to share an endpoint. The two studies are unusually well matched on the variables that typically drive cross-trial noise: identical acute-inpatient population and 5-week duration, identical primary endpoint (PANSS total at Week 5), nearly identical age range (18-60 vs. 18-64), identical diagnostic confirmation (DSM-5 + MINI), identical CGI-S severity threshold (≥4), and a majority of ZEPHYR’s investigative sites were also EMERGENT-1 sites. ZEPHYR is larger (307 vs. 182 patients, ~24 vs. 12 US sites) and adds a second active dose arm, but the population and operational infrastructure are substantially shared. That’s a stronger basis for calibration than the standard “different trial, different era” caveat usually allows.
A few differences are worth flagging rather than assuming away. EMERGENT-1’s protocol specified stricter symptom thresholds (PANSS 80-120, ≥2 positive-symptom items ≥4) and explicit exclusions, including treatment-resistant schizophrenia and cholinergic-relevant conditions (urinary retention, narrow-angle glaucoma, IBS, clinically significant constipation). ZEPHYR’s public registry describes eligibility more broadly (”moderate and persistent symptoms”) without listing these same exclusions — likely abbreviated registry reporting rather than a substantive design change, though it could also reflect greater sponsor confidence in ML-007’s peripheral tolerability. Worth flagging as open rather than resolved without the full protocol in hand.
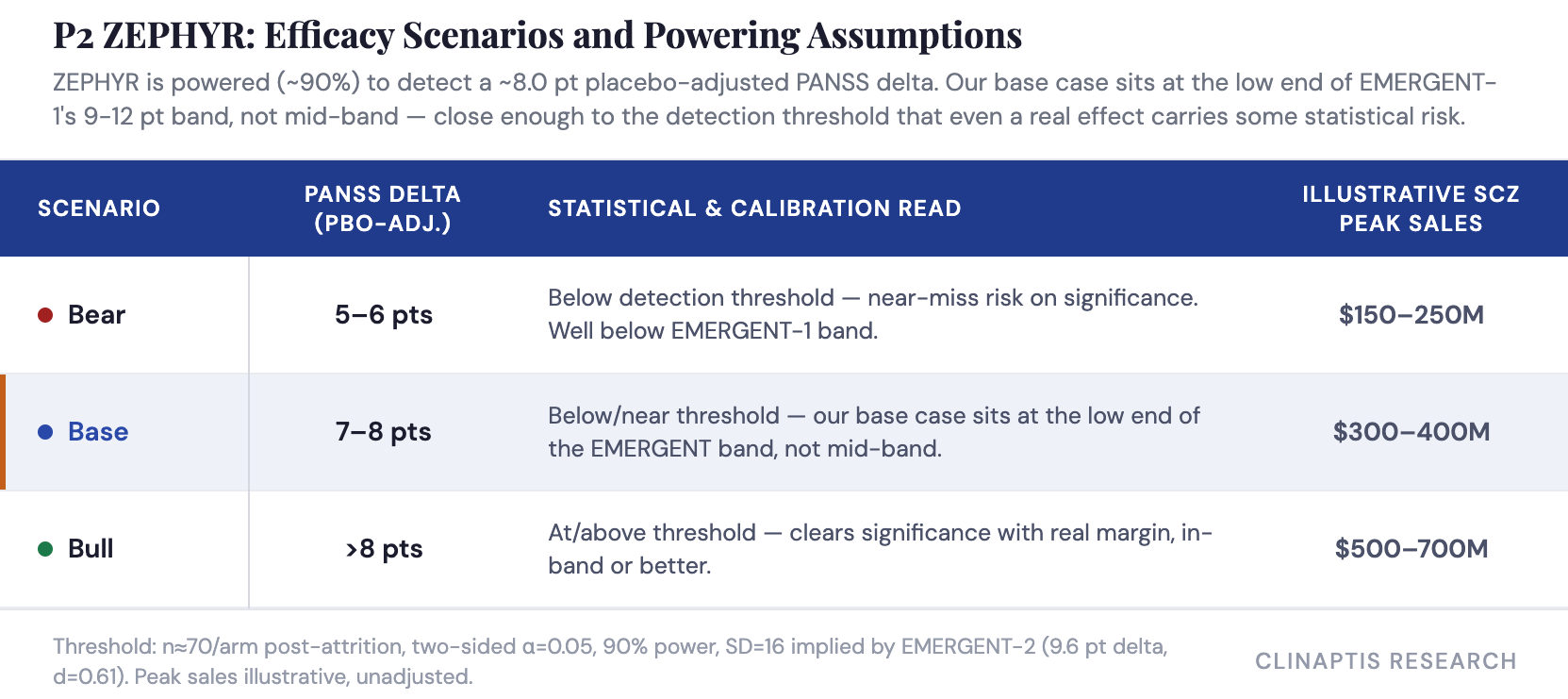
Given how closely matched the two trials are, a placebo-adjusted PANSS result in ZEPHYR falling within or near EMERGENT-1’s ~9-12 point range should read as clean replication, not an ambiguous one — the design similarity removes most of the usual excuses for a miss. To be clear, a base case at the low end of the EMERGENT band isn’t a comment on the mechanism or the molecule — it reflects our own read of the evidence, not a signal that something is wrong with ML-007C-MA. A modest, in-band result would still validate the platform; it just wouldn’t be the blow-out some investors may be underwriting at current levels. Efficacy replication is table stakes, though; the more important question, per Section III, is whether ML-007C-MA holds that efficacy alongside a genuinely differentiated tolerability profile.
Watch the Marder factors, especially negative symptoms. PANSS total drives the regulatory outcome, but the Marder negative-symptoms factor is the more interesting differentiation endpoint. D2 antagonists remain structurally weak against motivation, affect, and social withdrawal — the symptom domain most tied to long-term functional outcomes. Any meaningful separation here, even as an exploratory secondary, would impress on KOLs who put lot of weight on long term adherence.
The two-dose design provides built-in commercial optionality. Unlike EMERGENT-1’s single-regimen design, ZEPHYR tests 210/3 mg BID and 330/6 mg QD head-to-head against a shared placebo — letting MapLight select the Ph3 dose based on observed efficacy-tolerability balance rather than committing upfront. If QD dosing matches BID on efficacy with comparable or better tolerability, that’s a real, if modest, commercial edge through simpler outpatient dosing; a clear efficacy gap between the two would undercut the convenience argument instead. Which dose wins may end up mattering almost as much as whether the study is positive at all.
V. What’s Priced, What Isn’t.
The stock’s run-up already prices meaningful odds of success — and with IRIS now in rearview mirror, ZEPHYR carries the full weight of the August catalyst window alone. Because tolerability is the platform’s primary thesis, a weak readout doesn’t just hurt the schizophrenia case, it undercuts the bigger ADP opportunity too.
Stock Setup
Market cap: ~$1.74B; Cash ~$395M, runway into 2027, no financing overhang.
Momentum: up ~35%+ over the past month.
Options market: front-month implied vol ~143% (~99th percentile) — pricing a highly binary event.
Short interest: 12.1% of float (~1.68M shares), 6.8 days-to-cover — enough to amplify a post-readout move either way (lag of 10 days+).
We don’t think that binary pricing is unreasonable. ZEPHYR is ML-007C-MA’s first real proof-of-concept — the result de-risks (or doesn’t) both the Ph3 schizophrenia path and, by extension, VISTA’s shot at the larger ADP population, a sequencing that echoes Cobenfy’s own indication-expansion playbook. The setup is also cleaner than it might otherwise be: IRIS’s June miss already flushed out the “two independent shots on goal” optimism priced in earlier this year, so what’s running into August is ZEPHYR-specific conviction, not a blended bet across two uncorrelated catalysts. Investors we track across neuropsych generally lean positive into the print, though not emphatically so.
ZEPHYR isn’t being valued solely on schizophrenia economics. The larger strategic prize is Alzheimer’s disease psychosis (ADP), where VISTA reads out 2H27 against a market with no approved therapies and current off-label options carrying black-box mortality warnings.
Part of today’s valuation likely reflects the market treating ZEPHYR as a read-through for VISTA, not just a schizophrenia proof-of-concept — a dynamic that matters more now than it did earlier in the year, since IRIS’s June readout (a primary miss, with a narrower positive signal in a high-irritability subgroup) removed the second, uncorrelated catalyst.
That creates a real asymmetry. Because MapLight’s differentiation rests on peripheral tolerability, not new receptor biology, a weak ZEPHYR tolerability signal wouldn’t just dent the schizophrenia opportunity — it would weaken confidence in the platform thesis underpinning VISTA, MapLight’s larger long-term value driver. A clean efficacy-plus-tolerability result cuts the other way: validation extending well beyond schizophrenia alone.
VI. Bottom Line
The evidence assembled here supports a narrower, more credible version of MapLight’s thesis than its own marketing implies. This isn’t a story of eliminating cholinergic side effects — nausea remains common in the company’s own Ph1 data. It’s a story of shifting which side effects show up, built on a genuine mechanistic refinement layered on Cobenfy’s proven peripheral-blockade principle. That refinement has been tested so far only in small, dose-selected Ph1 cohorts, not the larger, more heterogeneous population ZEPHYR enrolls — and it’s priced with real conviction already, given the stock’s run into the catalyst.
What to watch on the day, in order of what actually matters:
The AE table, not the PANSS topline. Does vomiting, constipation, and anticholinergic incidence stay low at scale, or does the clean Ph1 profile — itself the product of discarding two less-favorable dose regimens — hold up in a larger, more heterogeneous inpatient population?
PANSS delta relative to ~8 points. Our base case sits at the low end of the EMERGENT band, close enough to ZEPHYR’s own detection threshold that even a real effect carries some statistical risk — this is the line that separates a clean win from an ambiguous one.
Which of the two doses wins, and whether QD dosing preserves both efficacy and tolerability — this shapes the commercial story as much as the topline result does.
A clean sweep across all three would be a materially different outcome than “PANSS replicated” alone — and the read-through wouldn’t stop at schizophrenia. Cobenfy proved the mechanism travels. ZEPHYR would prove the molecule does too.
Disclaimer: This note is published by Clinaptis for informational and educational purposes only. Nothing herein constitutes investment advice or a recommendation to buy or sell any security. Clinaptis is not a registered investment advisor or licensed financial professional. All data and market figures referenced are sourced from publicly available information including company filings, earnings transcripts, clinical trial publications, and regulatory disclosures. Where figures are triangulated or estimated, this is noted explicitly in the text. Readers should conduct their own independent research and consult a licensed financial advisor before making any investment decision.
Clinaptis publishes independent market structure commentary on pharmaceutical and biotech categories. All views are the author’s own.